What is Transferrin Iron Binding Capacity (TIBC)?
TIBC measures the blood's total capacity to bind and transport iron using transferrin, a protein produced by the liver. When iron stores are low, the liver produces more transferrin to capture as much circulating iron as possible, raising TIBC. When iron stores are adequate or elevated, TIBC tends to fall. It is typically measured as part of a full iron studies panel alongside serum iron, ferritin, and transferrin saturation.
Why does it matter for long-term health and wellbeing?
Iron transport is fundamental to oxygen delivery, energy production, and cellular repair. TIBC provides a complementary picture to ferritin. While ferritin reflects stored iron, TIBC reflects the body's active demand for more. A high TIBC alongside low ferritin and serum iron strongly suggests iron deficiency, even before anaemia develops. Conversely, a low TIBC may point to iron overload, chronic inflammation, or liver dysfunction. Monitoring TIBC as part of a broader iron studies panel supports early identification of imbalances that can affect cognition, endurance, and long-term wellbeing.
What's an optimal level of TIBC?
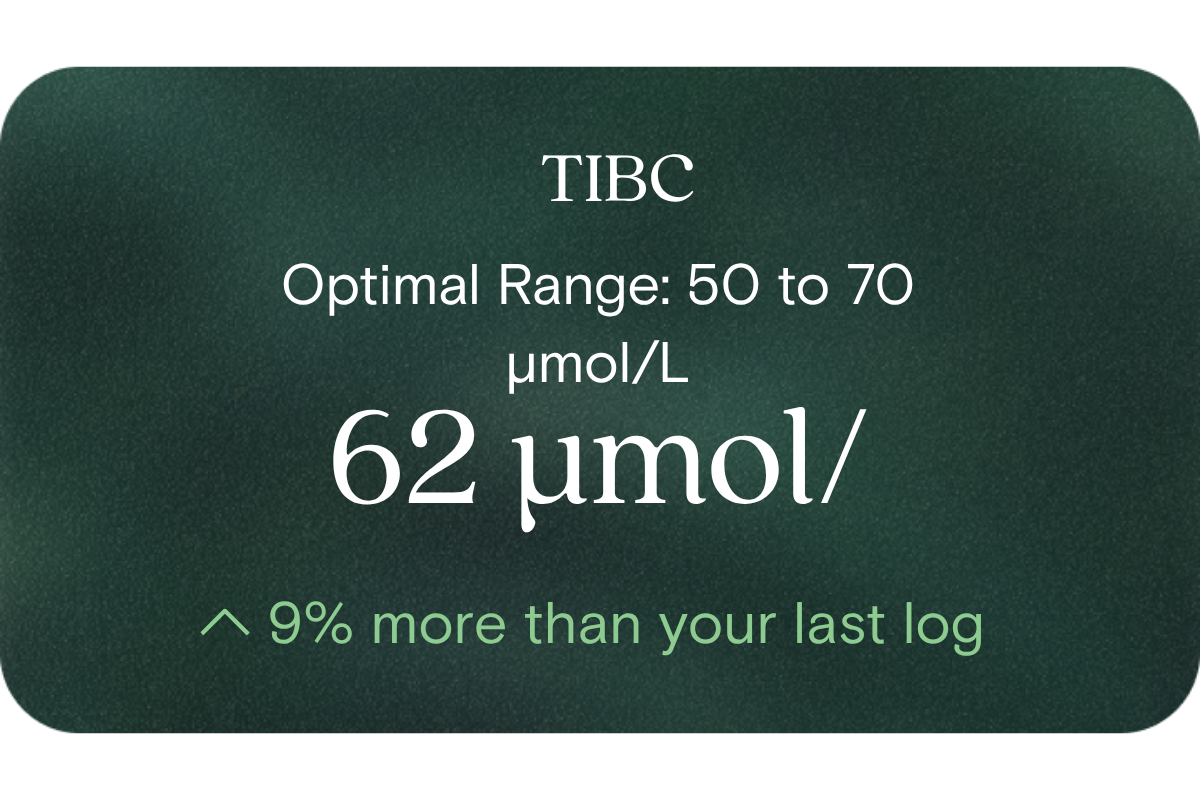
- Laboratory reference: 45 to 80 µmol/L
- Optimal (as per your framework): 50 to 70 µmol/L
- Note: Australian pathology labs typically interpret TIBC in conjunction with serum iron and transferrin saturation rather than in isolation.
What influences TIBC levels?
- Iron stores (low iron raises TIBC; high iron or overload suppresses it)
- Inflammation or chronic disease (tends to lower TIBC independent of iron status)
- Liver function (the liver produces transferrin, so hepatic conditions can affect TIBC)
- Nutritional status (protein deficiency and malnutrition can reduce transferrin production)
- Pregnancy (TIBC typically rises in pregnancy due to increased iron demand)
- Genetic conditions affecting iron metabolism, such as hereditary haemochromatosis
What does it mean if TIBC is outside the optimal range?
- Above optimal / high TIBC: Often indicates iron deficiency, as the body upregulates transferrin to capture more circulating iron. Most meaningful when accompanied by low ferritin and low transferrin saturation.
- Below optimal / low TIBC: May suggest iron overload, chronic inflammatory conditions, liver disease, or malnutrition. Low TIBC in the context of elevated ferritin warrants further clinical review.
How to support healthy TIBC levels?
- Address underlying iron deficiency through dietary sources (lean red meat, legumes, leafy greens) combined with vitamin C to enhance absorption
- Manage systemic inflammation through sleep, stress reduction, and an anti-inflammatory diet, as chronic inflammation independently suppresses TIBC
- Support liver health through limiting alcohol, maintaining a healthy weight, and eating a nutrient-dense diet
- Retest TIBC alongside serum iron, ferritin, and transferrin saturation to build a complete picture of iron status
- Consult a healthcare practitioner before supplementing iron, as supplementation without confirmed deficiency can cause harm
This information is provided for general health and wellness purposes only and does not replace medical advice.
References
- Royal College of Pathologists of Australasia. (2021). Iron Studies – Standardised Reporting Protocol (Second Edition). Surry Hills, NSW: Surry Hills, NSW: RCPA.
- Camaschella, C. (2015). Iron-deficiency anaemia. New England Journal of Medicine, 372(19), 1832–1843.
- Worwood, M. (2007). Indicators of the iron status of populations: ferritin. In Assessing the Iron Status of Populations (2nd ed.). World Health Organization.
- Trinder, D., Fox, C., Vautier, G., & Olynyk, J. K. (2002). Molecular pathogenesis of iron overload. Gut, 51(2), 290–295.















.png)

.svg)

