What are triglycerides?
Triglycerides are the main form of fat stored in your body and the most common type of fat circulating in your bloodstream. Each triglyceride is made up of three fatty acids attached to a glycerol backbone. They come from two sources: the fats you eat, and fats your liver produces from excess energy, particularly from refined carbohydrates, sugar and alcohol. Between meals, your body releases stored triglycerides for energy.
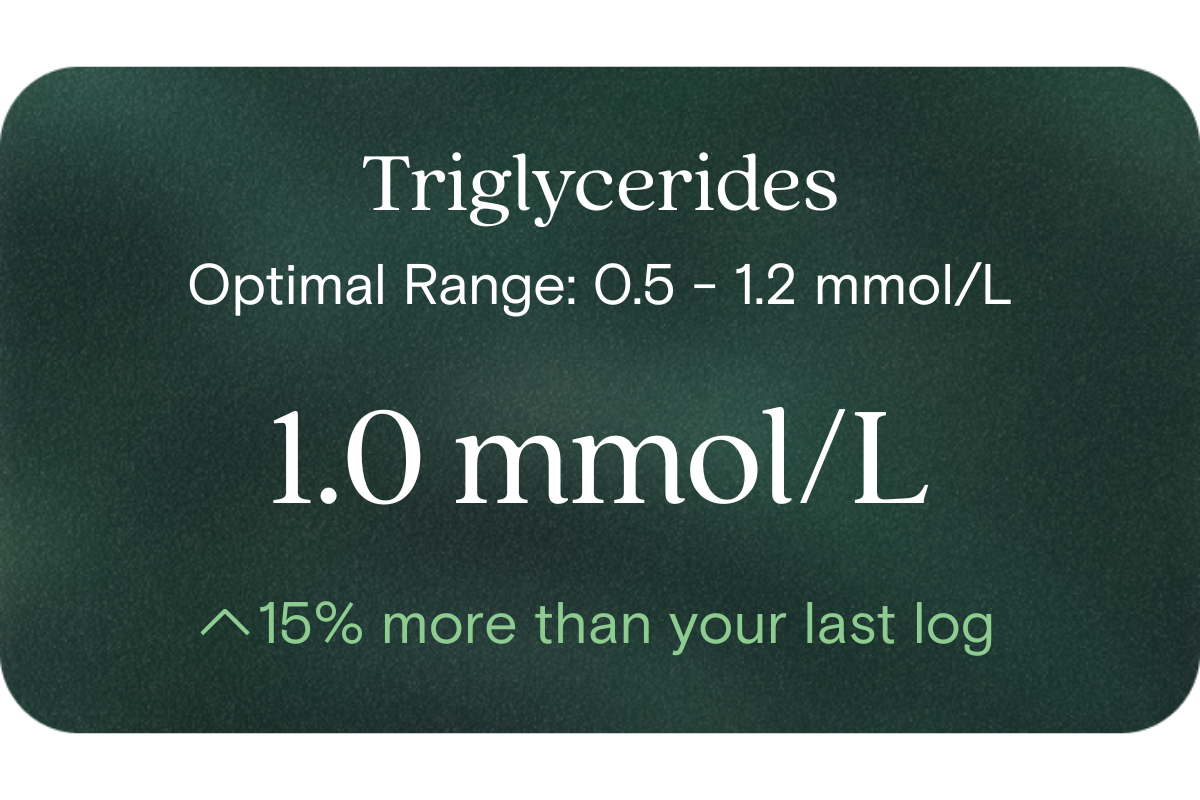
A triglyceride blood test measures the concentration of triglycerides in your blood, usually after a period of fasting, and is reported in mmol/L in Australia. It is a standard part of a lipid panel and one of the most useful markers for understanding both cardiovascular risk and metabolic health.
Why do triglycerides matter for long-term health and wellbeing?
Triglycerides are one of the most sensitive indicators of overall metabolic health. Elevated levels are strongly linked with insulin resistance, metabolic syndrome, non-alcoholic fatty liver disease, type 2 diabetes and cardiovascular disease. High triglycerides often reflect a diet high in refined carbohydrates, sugar or alcohol, along with excess visceral fat, and they typically travel alongside low HDL cholesterol and high blood glucose.
Very high triglycerides also carry a specific short-term risk: acute pancreatitis, a painful and potentially serious inflammation of the pancreas. Because triglycerides respond quickly to lifestyle change, they are one of the most actionable lipid markers to track over time. They are one of the core lipid markers Vively tracks as part of its baseline health testing.
What is an ideal triglyceride level?
In Australia, fasting triglycerides are generally interpreted as follows: below 1.7 mmol/L is considered optimal, 1.7 to 2.2 mmol/L is borderline high, 2.3 to 5.6 mmol/L is high, and above 5.6 mmol/L is very high and carries an increased risk of pancreatitis. For long-term metabolic and cardiovascular health, many clinicians prefer to see fasting triglycerides comfortably below 1.5 mmol/L, and lower still (around 1.0 mmol/L or less) when insulin resistance is a concern.
There is no single perfect number. Interpretation depends on your age, sex, fasting status, medications, other lipid markers, blood glucose, blood pressure and overall cardiovascular risk. Non-fasting triglycerides are naturally higher than fasting values and are increasingly used, though fasting samples remain the standard in Australia for most lipid assessments.
What influences triglyceride levels?
Diet has a strong and relatively quick effect on triglycerides. Refined carbohydrates, sugary drinks, sweets, ultra-processed foods and excess alcohol are among the biggest drivers of high triglycerides, often more so than dietary fat. Excess calories from any source can also lift triglycerides, since the liver converts surplus energy into triglycerides for storage. Meal timing matters too, as triglycerides rise after eating and can stay elevated for several hours.
Body composition, physical activity, sleep and stress all influence triglycerides. Insulin resistance, type 2 diabetes, hypothyroidism, chronic kidney disease and non-alcoholic fatty liver disease are common medical contributors, and genetics play a significant role for some people. Medications that can raise triglycerides include corticosteroids, oestrogen therapy including some oral contraceptives, tamoxifen, retinoids, some beta blockers, thiazide diuretics, some antipsychotics and some immunosuppressants.
What are the symptoms of high triglycerides?
High triglycerides usually have no symptoms and are typically discovered only through a blood test. This is one of the main reasons routine testing matters. When triglycerides are very high (generally above 10 mmol/L, and sometimes lower), symptoms can include upper abdominal pain, nausea, vomiting or acute pancreatitis. Very rare visible signs include yellowish fatty deposits on the skin (eruptive xanthomas), a whitish appearance in the blood vessels of the retina (lipaemia retinalis), or a milky appearance to the blood itself in laboratory samples.
More commonly, high triglycerides sit within a broader pattern of metabolic dysfunction that can include stubborn abdominal weight gain, fatigue, energy dips after meals and sugar cravings. Our article on how to tell if you are insulin resistant explains this pattern in more detail.
What causes high triglycerides?
The most common causes are lifestyle-related: a diet high in refined carbohydrates, sugary drinks, alcohol and ultra-processed foods, excess visceral fat, low physical activity, poor sleep and chronic stress. Insulin resistance is a major underlying driver, which is why high triglycerides so often appear alongside low HDL, high blood glucose and features of metabolic syndrome.
Medical conditions that can raise triglycerides include type 2 diabetes, non-alcoholic fatty liver disease, hypothyroidism, chronic kidney disease, nephrotic syndrome and some inherited lipid disorders. Pregnancy naturally raises triglycerides, particularly in the third trimester. Medications such as corticosteroids, oestrogen-containing therapies, retinoids, some beta blockers and some antipsychotics can also lift triglyceride levels.
What are the symptoms of low triglycerides?
Low triglycerides in a healthy person are generally not a concern and often reflect good metabolic health, particularly when other lipid and glucose markers are also healthy. If very low triglycerides occur alongside an underlying condition, symptoms tend to relate to that condition rather than to the triglyceride level itself. For example, an overactive thyroid can cause weight loss, palpitations and heat intolerance, while malabsorption might present with digestive symptoms, weight loss or nutrient deficiencies.
If your triglycerides are unexpectedly low, particularly alongside other unusual results, your GP will consider the broader clinical picture rather than the number in isolation.
What causes low triglycerides?
For most people, low triglycerides simply reflect a healthy diet, healthy body composition and good metabolic health. However, several medical conditions can lower triglycerides more than expected. These include hyperthyroidism, malnutrition, malabsorption disorders such as coeliac disease, chronic liver disease, some cancers, prolonged fasting and extreme calorie restriction. Certain rare genetic conditions can also cause very low triglycerides from an early age.
Some medications used to treat high lipids, such as fibrates, statins and omega-3 prescription therapy, can lower triglycerides, which is generally the intended effect. As with any marker, low results are best interpreted in the context of your overall health, symptoms and other test results.
What does it mean if triglycerides are outside the optimal range?
A higher-than-optimal triglyceride level suggests your body is dealing with more circulating fat than it can efficiently clear, often due to a combination of diet, lifestyle and insulin resistance. It does not diagnose diabetes, fatty liver or cardiovascular disease on its own, but it increases the likelihood of these conditions and often signals broader metabolic strain. Very high triglycerides (typically above 5.6 mmol/L) require prompt medical attention due to the risk of pancreatitis.
A low triglyceride level is usually reassuring, though very low values without an obvious lifestyle explanation may occasionally point to an underlying condition worth investigating. As with all lipid markers, patterns over time and the context of your other results matter far more than any single reading.
Can triglycerides be normal but something still be wrong?
Yes. A single normal triglyceride result does not always rule out metabolic dysfunction. Triglycerides fluctuate significantly throughout the day and are very sensitive to recent food, alcohol and even a couple of good or bad weeks of eating. A single sample after a lighter-than-usual few days can look better than your typical pattern.
You can also have normal triglycerides alongside high LDL, elevated ApoB, high Lp(a), high blood glucose, elevated fasting insulin or inflammation, any of which can drive cardiovascular and metabolic risk independently. This is why triglycerides are best interpreted alongside a full lipid profile and metabolic markers, as explored in our article on advanced lipid testing beyond LDL cholesterol.
What other markers should be checked with triglycerides?
Triglycerides are most useful as part of a full lipid profile. HDL cholesterol is a key companion, and the triglyceride to HDL ratio is a widely used simple proxy for insulin resistance and small, dense LDL particle burden. LDL cholesterol, non-HDL cholesterol and the total cholesterol to HDL ratio add further cardiovascular context, as covered in our guide to the total cholesterol to HDL ratio.
Because triglycerides are so closely tied to metabolic health, checking fasting glucose, HbA1c, fasting insulin and the HOMA-IR index gives valuable insight into insulin resistance. Liver enzymes such as ALT and GGT help flag fatty liver disease, hs-CRP captures low-grade inflammation, and uric acid often rises with metabolic syndrome. ApoB and Lp(a) add depth for cardiovascular risk assessment. Blood pressure, waist circumference and family history are also essential context. You can see the full set of markers Vively looks at through our tests page and shop tests page.
How can you improve triglycerides to a healthier level?
Triglycerides are one of the most responsive lipid markers to lifestyle change. Reducing refined carbohydrates, sugary drinks, sweets and ultra-processed foods usually lowers triglycerides quickly. Cutting back on alcohol is one of the fastest ways to bring high triglycerides down, since alcohol is a strong driver. Prioritising unsaturated fats from olive oil, nuts, seeds, avocados and oily fish, along with plenty of vegetables, legumes and fibre-rich whole grains, tends to support healthier levels.
Regular movement helps significantly, especially aerobic exercise, strength training and post-meal walks. Improving body composition, particularly reducing visceral fat, is one of the biggest levers. Quality sleep, stress management and treating underlying conditions such as hypothyroidism or diabetes also matter. For persistently high triglycerides, especially very high levels, medications such as fibrates, high-dose prescription omega-3 or statins may be recommended by your GP. Vively's how it works page explains how testing, monitoring and dietitian coaching combine to make change practical.
When do triglycerides need medical review?
See your GP if your triglycerides are persistently elevated, are rising over time, or are above 5.6 mmol/L, which carries an increased risk of pancreatitis and often needs prompt treatment. Any symptoms such as severe upper abdominal pain, nausea or vomiting alongside high triglycerides should be reviewed urgently.
Clinical review is also important if high triglycerides appear alongside diabetes, PCOS, fatty liver disease, cardiovascular disease, chronic kidney disease or hypothyroidism, or during pregnancy and when planning pregnancy. Very low triglycerides without a clear reason are worth discussing too. Triglycerides should never be self-diagnosed, as they are one piece of a bigger clinical picture your GP or cardiologist can help you interpret through an absolute cardiovascular risk assessment.
How does Vively help you understand triglycerides?
Triglycerides are one of the lipid markers included in the Vively Baseline Health Check, alongside LDL, HDL, non-HDL, cholesterol ratios, ApoB, Lp(a) and more than 60 other biomarkers spanning metabolic, liver, kidney, inflammation and hormonal health. Rather than looking at triglycerides in isolation, Vively interprets them in context with your other results, symptoms, lifestyle and family history.
A registered nurse reviews your results with you one on one, and accredited practising dietitians support the changes that follow. Because your markers are retested over time, you can see how nutrition, alcohol, movement, sleep and other habits are shifting your triglyceride level and broader lipid profile rather than guessing. Start at the Vively homepage or explore the full range of tests in the Vively shop.
References
- Heart Foundation of Australia. Australian guideline for assessing and managing cardiovascular disease risk. https://www.cvdcheck.org.au/
- Royal Australian College of General Practitioners. Guidelines for preventive activities in general practice (Red Book). https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/red-book
- Royal College of Pathologists of Australasia. RCPA Manual: Lipids. https://www.rcpa.edu.au/Manuals/RCPA-Manual/Pathology-Tests/L/Lipids
- Healthdirect Australia. Cholesterol. https://www.healthdirect.gov.au/cholesterol
- Better Health Channel, Victorian Department of Health. Cholesterol. https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/cholesterol
- Heart Foundation of Australia. Blood cholesterol. https://www.heartfoundation.org.au/your-heart/blood-cholesterol
- Australian Institute of Health and Welfare. Heart, stroke and vascular disease: Australian facts. https://www.aihw.gov.au/reports/heart-stroke-vascular-diseases/hsvd-facts
- Miller M, Stone NJ, Ballantyne C, et al. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123(20):2292 to 2333.
- Nordestgaard BG, Varbo A. Triglycerides and cardiovascular disease. The Lancet. 2014;384(9943):626 to 635.
- Cleveland Clinic. Triglycerides. https://my.clevelandclinic.org/health/diagnostics/17583-triglyceride-test
- Mayo Clinic. Triglycerides: Why do they matter? https://www.mayoclinic.org/diseases-conditions/high-blood-cholesterol/in-depth/triglycerides/art-20048186
- National Institutes of Health, MedlinePlus. Triglycerides. https://medlineplus.gov/triglycerides.html















.png)

.svg)

